James M. Roe, et al. – University of Oslo.
Background: Previous studies of whether AD risk genes affect age-related changes in brain structure have yielded mixed results, often employing cross-sectional data.
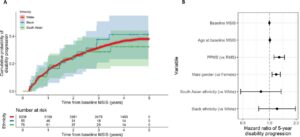
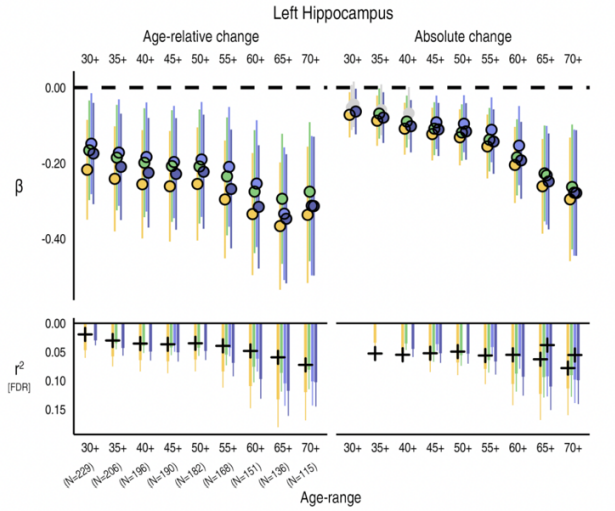
This Study: Examining data from a cohort of healthy (non-AD, defined as MMSE >= 25) adults assessed over decades, Roe and colleagues found that subjects with elevated polygenic risk scores for AD (PRS) experienced greater declines in volume of the hippocampus, particularly left hippocampus, and left amygdala than other subjects of the same age. These changes in brain volume remained significant after controlling for APOE genotype, indicating that these findings were not just the product of this highly-potent risk gene. Given that the MMSE is the sole criterion used to exclude AD, it remains possible that some subjects would be classified as experiencing prodromal AD by other measures.
Of the 4 PRS systems used in this study, most significant results came from that described by Jansen et al 2019, suggesting that that study may have uniquely captured genes linked to aging-related brain changes. Additionally, using a metric that encompasses numerous regions that distinguish patients with AD from controls, healthy subjects with higher PRS showed greater deficits, though the effects were more dependent on APOE genotype.
Bottom Line: Existing metrics for PRS may be identifying factors linked to aging-related decline, rather than AD-specific decline.